Even though this Stop the Thyroid Madness blog, website and the books pertain to thyroid patients and their issues, it’s been observed that many thyroid patients have also found themselves with high copper, whether from low zinc due to illness, the MTHFR or other methyl mutations, chronic high stress, mold exposure (which can tank zinc), high estrogen, the use of a copper IUD, or other causes.
Even though this Stop the Thyroid Madness blog, website and the books pertain to thyroid patients and their issues, it’s been observed that many thyroid patients have also found themselves with high copper, whether from low zinc due to illness, the MTHFR or other methyl mutations, chronic high stress, mold exposure (which can tank zinc), high estrogen, the use of a copper IUD, or other causes.
I am one who found myself with high copper.
*****************
My story
Looking back, I’m fairly certain my high copper was manifesting itself in Fall of 2014 by suddenly developing very weird iron labs. My serum iron plummeted from 103 down to 55 in just one week of high physical activity. Huh?? I’d get it back up, then down it would fall.
Turns out that high heavy metals can mess with your iron levels—others might see low ferritin with high iron. I also started to notice movement headaches in the Fall of 2014, and I’m not a headache person, so that was new. In October of 2014, I did hair testing and though copper was midrange, It should not have even been mid-range, but I didn’t understand the significance.
In early 2015, I was seeing my hair come out in clumps, yet I had gotten my iron back up once again. Finally in March of 2015, I was noticing I had ruminating negative thoughts--not at all like me!! What the heck was this about??
How my labs revealed a copper problem
First, the clue that a problem was brewing was shown in October 2014, but I didn’t understand the significance. i.e. it was the metals hair testing, called an HTMA, showing Copper was going up at 23 (11-37). This is the one I ordered and did: https://www.directlabs.com/sttm/OrderTests.aspx
By April of 2015, my symptoms were so horrible in my BRAIN that I did serum testing of copper and zinc. And there it was: high copper, relatively low serum zinc—they have a see-saw relationship! Another important test is hair testing, also since not everyone is lucky with blood testing as I was. Finally, a good indication is high calcium, which I had and is called the calcium shell, but didn’t know the connection to high copper!
Additionally, a Calcium result was SUPER high 1840 (300-1200) which correlates to rising copper. It’s called a Calcium Shell, meaning a high tissue level that that forms to protect against stress. That should have screamed at me, but I wasn’t informed.
Here are my lab results in April 2015.
Copper, Serum: 1.36 mcg/mL (.75 — 1.45) HIGH
Zinc, Serum: .81 mcg/mL (.66 — 1.10) LOW (And if only I had done the RBC zinc!!)
Ratio: 1.68 (should be .7 — 1.0) TOO HIGH
Ceruloplasmin: 40.5 mg/dL (16 — 45) (this is the protein that binds and carries copper around)
Bound Cu: 121.5, Unbound Cu: 14.5 (optimal unbound Cu: 5-15)
% Unbound Cu: 10.7% (optimal 5-15%)
*** Note that I did serum copper and zinc—some will say it needs to be plasma, but serum confirmed it anyway as did my symptoms. Others recommend Copper RBC and Zinc RBC, and I would now do the RBC zinc, not the serum.
What caused my high copper
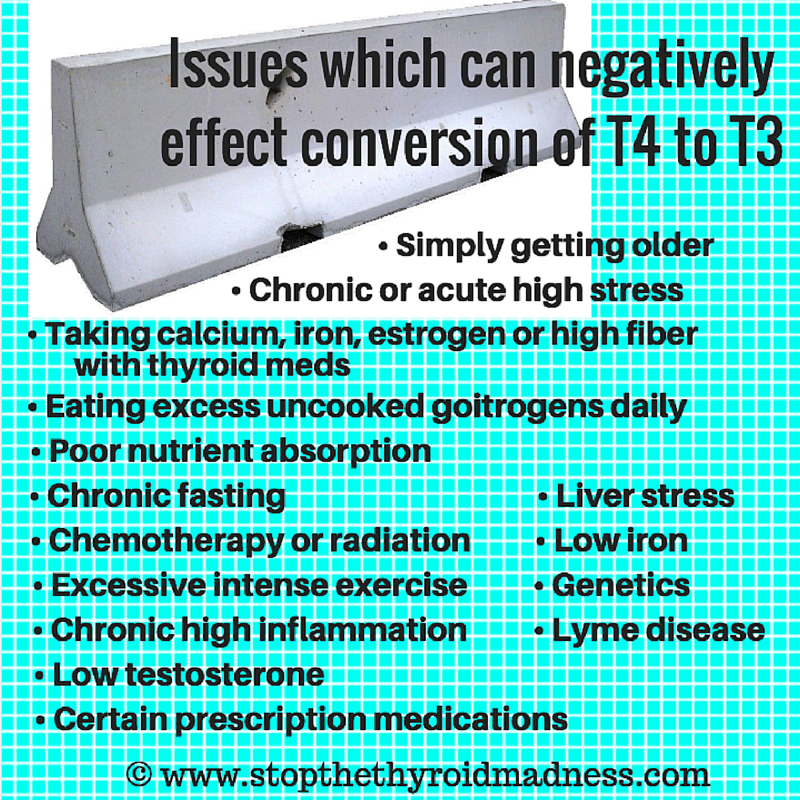
I’m fairly certain it was because 2014 was a year of constant and unrelenting high stress, both good and bad. I was editor of the STTM II book, plus had many other things going on in my life—good things, but chronic and stressful. And turns out that chronic high stress can deplete your zinc, which in turn can cause copper to rise.
Additionally, I was recovering from mold inhalation, which left me quite sick the year before. Not only is mold stated to lower zinc, but my immune system was in high gear battling it, and that can also tank nutrients like zinc. (You will see later in this article that only in 2017 did I discover my RBC zinc was BELOW range)
On top of the stress/mold zinc fact, I was eating a huge amount daily of stevia-sweetened dark chocolate daily as my way of self-comforting myself through the unrelenting stress. And chocolate is high copper! I was unknowingly feeding my internal levels of copper that were destined to climb in the face of my low zinc.
Additionally, I found out later the next year via hair testing that I had low levels of both manganese and chromium–another inducement of rising copper. Some literature states that deficient levels of B-vitamins and vitamin C can also promote rising copper levels–I had both deficiencies but didn’t know it at the time.
How I started the detox
This is where there is all sorts of strong opinions in groups, so I had to do careful reading make a decision for myself.
- The most important step I took is to get off of all high copper foods. That especially included all the stevia dark chocolate I had been consuming to self-treat stress. Bad mistake when zinc was so low. (I initially left this step off when I created this page, and shouldn’t have. It’s the most most important step!)
- I got on Manganese and Molybdenum (not even knowing I was low in both, as I found out later). Manganese is stated to help remove copper, especially from the liver. Molybdenum is stated to bind to copper and greatly facilitates its excretion.
- I also got on B-vitamins, especially b6 and zinc to start detoxing. But I had to learn the hard way that the b’s heightened the speed of my detoxing (and fatigue misery) and I had to take MUCH lower amounts. I may be a fast metabolizer.
- Some will say take no zinc whatsoever, but my experience is that low levels were fine.
- I was also taking curcumin and astaxanthin for inflammation
- To support my liver and kidneys (the detoxing glands), I used Milk Thistle (but use iron with it–it can lower iron levels) plus Dandelion Root, plus Swanson’s Kidney glandular. P.S. I also detoxed a second time starting June, 2016)
My detoxing experience
I started detoxing in late April 2015, and it ended on its own by October 2015. And frankly for ME (though it may not be this bad for you), it was absolutely miserable with fatigue and weakness. I was completely exhausted the entire time in an extreme way—much worse than I read in others.
BUT, I later figured out that for whatever reason, I wasn’t breaking down carbs well to give me energy to endure the detox. And the latter was due to the fact that my pancreas wasn’t releasing enough of the enzyme called amylase which breaks down starches and carbs for energy! My situation was probably rare.
But one thing did help back then before I knew about my low-amylase caused low energy: CoQ10! I got on 1500 mg liquid Ubiquinol daily. That did help! Because all the stress I was going through at the time also caused super high Succinate, Fumarate, Malate and a-ketoglutarate in my urine as revealed by an Organic Acids Test (OAT)–implying I had an energy metabolism disorder.
Ironically, though my body stopped detoxing on its own as I neared six months, and though my serum zinc levels were fabulous now, my serum copper was still a little too high. But I redid hair testing, and things were good enough there in my mind i.e. 16 (11 — 37). That was far better than the previous mid-range of 23–and which I have no doubt got MUCH higher before I caught it all (In hindsite, I found out my probably should have detoxed more. That came in 2016)
Did the high copper affect my emotions and brain?
It sure did. I had movement headaches in late 2014 before I ever knew about my rising copper i.e. if I bent down to pick up something, there it was. Right before I started to detox the first time in April 2015, and when my copper had to be sky high, I noticed I had ruminating fearful negative thoughts. My brain must have been loaded with copper by then, as copper is a known neurotoxin. The second time around in 2016, and as I was entering the third month of detoxing, I noticed depression was creeping in, irritability, impatience. I can imagine that the latter is related to the copper moving around to be released.
Did the high copper and especially the detox effect my thyroid?
Yup. It sent my reverse T3 (RT3) up, which is probably due to the inflammation levels it pushed up. I had to be on mostly T3 instead of the natural desiccated thyroid (NDT) I had been on.
Was I able to keep my copper levels down after detoxing?
Unfortunately, no. There was evidence that it went back up. Because in the Spring of 2016, I was seeing more hair loss than normal again, yet my iron was great. No, I didn’t have the movement headaches or the ruminating negative thoughts like I did the year before, but the hair loss was a sign. Then at the beginning of June 2016, my body started detoxing copper again! I wasn’t trying to do so—it happened from taking phospholipids, known to help heal the mitochondria (of which I had a problem as revealed by the Organic Acids Test and symptoms—not everyone does). But it turns out that phospholipids induce detoxing! So here I was, once again detoxing copper with the exact same symptoms I had in 2015—copper-colored stools, adrenal stress, fatigue. It all lasted nearly 6 months again. The two phospholipids were NT Factor and Body Bio—one in the morning and one in the evening. Some just use NT Factor.
Then it happened again in 2017, but luckily only a month. And you know what started the detox this time? Trying out 10 mg of lithium instead of 5. I was using low dose lithium to help get B12 to my cells better.
And then, again in April 2018–very strongly as revealed by the stools and fatigue. But this time, I was prepared, and taking many adrenal-calming supplements helped a lot in that area. I also went back up on my ubiquinol.
Why the continual copper detoxing? One clue is the excessively high amount I had–some literature says it can take a few years to get it all out. That seems true to my experience.
What did 2017 reveal about my zinc?
All through 2015 and 2016, I was always doing serum zinc labs. In April of 2015, when I first understood I had a serious Copper problem, it was LOW: .81 (.7-1.10). I got it towards the top of the range by the end of 2015, and did so in 2016 and worked to maintain that.
But in the Fall 2017, I did an RBC zinc instead of serum: BELOW RANGE. RBC stands for red blood cells. Seeing BELOW range threw me against the wall in shock: I may have had below range RBC zinc ALL this time. No wonder I had a copper problem!! I was already on 30 mg zinc, and I went to 80mg zinc. THAT is one way we can all control our levels of zinc–keep it up!
What about the MTHFR mutation in all this?
Since the MTHFR mutation can contribute to high heavy metals, there is a question if my single 1298 heterozygous mutation may have contributed, or my other methyl mutations like COMT. I’ve seen that happen to others. So just in case, I stay on folate plus other B vitamins.
What are surprises I had during the entire high copper journey?
My biggest one was finding out that not only did I have high copper, I also had high lead (though not as high as the copper). Both were revealed by the hair testing I did in 2014…and both came down after those six months of detoxing in 2015 as also revealed by another hair test.
The second surprise was discovering that copper detoxing (or high copper) can cause SIBO, Small Intestinal Bacterial Overgrowth. Have never had gut problems in my life, then found myself with SIBO that I had to treat. (Turns out SIBO can happen due to a poor release of bile from the gallbladder!) The third surprise was that I started to detox again in 2016 by accident!
And the final surprise?? Finding out why this may have all happened in the first place. My RBC zinc was BELOW range in 2017, that means it had to have been horridly low by 2014—-all due to my immune system in high gear in 2013 due to mold poisoning. Immune systems need a lot of nutrients to be effective.
Copper-color stools when detoxing–really??
Absolutely! It happened when I detoxed for six months in 2015 (and went away once my body stopped), happened exactly again when I started to detox in 2016, and happened in 2017 and 2018 for shorter, but still challenging, detoxes.
If I could change/improve anything about my high copper experience, as well as detoxing, what would that be?
- I find the biggest emphasis should be on supporting your natural detox organs like the liver, kidneys and skin. If you do a sauna to sweat out the metals, it’s the skin helping you. But I tended to support my liver (Milk Thistle for one) and kidneys (Swanson Kidney Extract twice a day) during the second round of detox. Why? Because I tend to naturally detox with the elimination organs!
- I find it quite important to take key antioxidants when detoxing like Astaxanthin, Grape Seed Extract, Vit. C and E, etc. I didn’t get into that well enough the first time around and regret it, so I did much better using them the second time around.
- It’s going to be quite important to find out if you have the MTHFR mutation causing high heavy metals and treat it. I don’t think this was my cause, but it would be for you, especially if you have the 677 MTHFR mutation.
- With what I know now, I would be on high amounts of CoQ10 (ubiquinol, not ubiquinone) while detoxing to support my mitochondria. I did that for the second detox and felt a little better. But you may not have the energy metabolism issues I had as discovered via the Organic Acids Test. I also discovered via a stool test that I have an intermediate level of carbs in my stool–a carbohydrate metabolism disorder. I don’t uptake carbs well for energy! No wonder I was so exhausted with detoxing!
- I should have been on glutathione…a master antioxidant in your body. It was used up by all this detoxing and exposure to toxins, and I didn’t even find THAT out until January of 2019. UGH. I used infusions to get it up. No wonder I noticed myself aging quicker!
Did detoxing effect my adrenals in any way?
Boy did it. Detoxing heavy metals can be a huge stress on one’s adrenals! Now understand that I did NOT have an adrenal issue before I started detoxing. So at the beginning of detoxing, I didn’t even think about it. But as it continued, it became clear that my cortisol was shooting high. I started to have sleep issues through the night. I felt shaky in the morning (adrenal excess can go with high cortisol just as it can with low). And around dinner time later in my detoxing, I had the internal buzzing feeling that can go with a cortisol issue.
The second six month detox I went through brought on high cortisol again—sleep issues, morning adrenaline and shakiness, evening same. What was effective for me was to take Holy Basil in the morning, again in the late afternoon if I noticed symptoms, and before bed. A side note: during the second detox, and after 4-5 weeks of my mitochondrial treatment with high-dose CoQ10 and B-vitamins, and my cortisol issue mostly went away. I also learned to take supportive adrenal supplements like Taurine, GABA, holy basil, ashwagandha, rhodiola….etc.
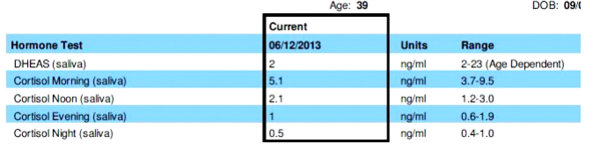
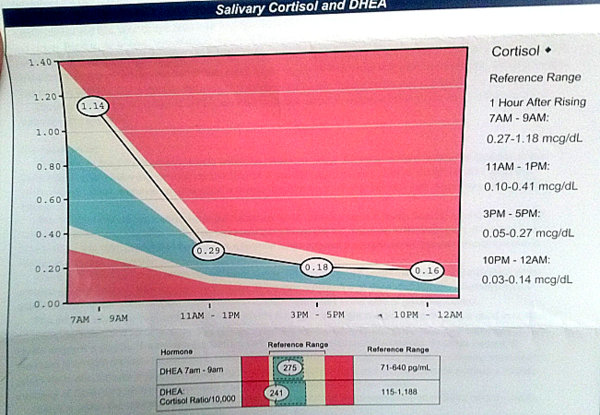
Want to know if your adrenals are being affected? You can order your own saliva cortisol test here.
Other bits of info
- Once I start detoxing, my body is simply going to continue it on its own no matter what. I must be a super detoxer.
- If there is excess fatigue with detoxing, look at your mitochondrial function via an Organic Acid Test (OAT). I am thinking my mito were functioning less than optimal before my 2015 detox, and the detox plus the SIBO plus a yeast infection from hell….ruined my mito. I took a very high dose of CoQ10, and added in NADH, along with the other supplements that the OAT told me about.
- I got a lot of good information from these websites: http://www.drlwilson.com/articles/copper_toxicity_syndrome.htm and http://www.coppertoxic.com/
- Use your best judgment after reading several sources. Be wise within any copper groups, as you will have to sift through strong opinion vs valid information and decide what fits you.
- This is the hair testing I have used twice, also called HTMA, and I will use it again to keep track of where my metals are: https://www.directlabs.com/sttm/OrderTests.aspx (3rd test down)
- Testing via blood should always be copper, RBC zinc and ceruloplasmin at the least (ceruloplasmin is the major copper-carrying protein). If ceruloplasmin is quite low or below range, might want to explore Wilson’s disease.
- It’s rare, but there are some who might have Wilson’s disease, which is an autosomal recessive inherited disorder. It causes accumulation of copper in major organs like your liver (failure to filter it out), brain, and more. www.wilsonsdisease.org/ That was not my cause, but you should read about it, just in case.
- About zinc and how it can be depleted: http://drlwilson.com/Articles/ZINC.htm
- TEST YOUR RBC zinc!!
- About ceruloplasmin: http://www.clinchem.org/content/51/8/1558.full
- Since high levels of copper is usually in the unavailable unbound form, you might see problems with yeast/candida.
- Also going hand-in-hand with high copper is high calcium, called the “calcium shell”. With that high calcium can be lack of emotion/apathy.
- High copper can also cause excess fears or anxieties. Detoxing may create some of the same. That happened to me. Could also be related to the adrenal stress it all causes.
- You will see ceruloplasmin mentioned on key copper websites—the major copper-carrying protein. Some will state that the lower it is, the quicker copper will build up in your liver and brain. Janie had high ceruloplasmin and still an obvious brain buildup! Just to show that there can be exceptions to the rule, it seems.
- If you want to work with a doctor, find one who is open-minded about hair testing aka HTMA. But you may be lucky and the blood testing shows the problem anyway along with symptoms. Want to order your own HTMA?? You can! Go to the following page, scroll down and click on the DIRECT LABS icon, and the hair test is the 3rd one down: www.stopthethyroidmadness.com/recommended-labwork
- Copper IUD’s have caused many women problems with rising copper levels! That can especially be true if you have the MTHFR mutation or even high stress.
- It’s stated that vegetarians have a high risk of becoming copper toxic.
- Foods high in copper include chocolate (darn it), avocados (darn it again) molasses, liver, oysters, shrimp, mushrooms, sesame or sunflower seeds, cashews, etc. A more comprehensive list is here.
PLEASE WORK WITH AN INFORMED DOCTOR IF YOU CAN FIND ONE.
If you found yourself with high copper, let us know your story by commenting below!
UPDATE FROM JANIE, late NOVEMBER 2016
Here is what I got down to in Sept. 2015 when I suddenly stopped detoxing following 5 1/2 months:
COPPER: 1400 (810-1990) (I was 1571 after detoxing two months)
ZINC: 1.09 (.66 — 1.10)
RATIO: 1.0 (you want it to be .7 — 1.0)
And here is where I am in late November 2016, after 5 1/2 months of detoxing high copper once again
COPPER: 1400 (810-1990)
ZINC: 130 ug/dL (60-130)
RATIO: 1.0 (you want it to be .7 — 1.0)
You can see they are nearly identical, each after detoxing 5 1/2 months. Zinc was a different measurement above, but at top of the range, just as last year.
And, with both detoxes:
1) High inflammation
2) High RT3, needing T3-only
3) Massive easy fatigue (I think both detoxes heavily messed with my mitochondria—the powerhouse of energy
Why test RBC levels of certain minerals? Because it’s measuring the intracellular levels in your body, which is even more important than serum levels. What can mess up your cellular levels? Toxic levels of other metals, for one. Those minerals which can have the RBC tested include Zinc, Copper, Potassium, Vanadium, Chromium, Manganese, Potassium, Selenium and Magnesium. The other metals need more then RBC, such as hair testing, i.e. they can be good with RBC, but high in hair. More good info here.
UPDATE FROM JANIE, late NOVEMBER 2018
Looking back, I have figured out that the stress of copper detoxing over the past few years may have contributed to gallbladder problems. The clues? The first one was having SIBO after my first detox in 2015–it’s strongly related to your gallbladder and bile levels. The second? I don’t break down fats well at all anymore. And there are other TMI clues that you can see by researching “symptoms of a sluggish gallbladder”. I have some; not all. But it’s very obvious. So I’m now taking Cholacol by Standard Process to help break down fats and which provides more bile. There are also things to be done to support a sluggish gallbladder, which you can also do an internet search for.
ADDITIONAL READING:
- This is a great read about what high copper can do to you: https://healdove.com/alternative-medicine/Hypercupremia-High-Copper And also note in the latter article that high copper can mess with your Glutamate/GABA balance, i.e. resulting in high glutamate levels in your brain (causing inflammation), plus in some, impaired speech, aggressive behavior, intense irritability, anxiety, inflammation of the gastrointestinal tract (GIT), and eventually neuronal destruction.
- Great website on the copper issue: https://coppertoxic.com/


 Summary: A working Natural Desiccated Thyroid, or adding T3 to that T4 as a second choice and getting those frees optimal, is a much better way to go than being on nothing but T4, according to years of worldwide patient experiences
Summary: A working Natural Desiccated Thyroid, or adding T3 to that T4 as a second choice and getting those frees optimal, is a much better way to go than being on nothing but T4, according to years of worldwide patient experiences