A healthy heart happens with T3 in the mix, report both patients and research!

*Did you know that your heart needs the thyroid hormone T3 to function well? That’s one of many reasons a healthy thyroid gives us direct T3.
*Did you know that some heart surgeons outright prescribe T3 to their heart patients?
Now granted, one could have inherited a heart problem of any kind due to genetics, or there can be other reasons you need to discover as the cause. So it’s important to go with your doctor’s guidance!
But many hypothyroid patients have discovered that their heart issues were directly related to being hypothyroid, or having problems with their cortisol levels contributing to continued hypothyroidism. Even low iron raises RT3, which makes you more hypothyroid.
Janie’s mother was a good example
I had never heard of anyone in my family of origin who had heart disease…until my mother, who was on nothing but T4 like Synthroid, found herself with clogged arteries, high blood pressure and a rising pulse. In her 60’s, she had to have an angioplasty. I remember thinking how odd the entire scenario was…until several years later when I became a Thyroid Patient Activist!
Turns out that the risk of heart-related problems and coronary heart disease can go hand-in-hand with either undiagnosed thyroid problems, or the use of Synthroid or Levo (which ends up leaving millions hypothyroid like my mother! Even being undertreated with T3 in your treatment can do it.
And that was my mother: treated with Synthroid (T4-only) her entire life, which we now know leaves all-too-many with lingering hypothyroid symptoms of our own degree and kind. She suffered from depression, poor stamina, afternoon fatigue, dry skin, dry hair…and finally culminating in the above. Bingo. Being forced to live for conversion alone (of T4 to T3) has harmed quite a lot of people, sooner or later, just like my mother.
And with patients being dosed by the TSH lab test (which we know leaves us hypothyroid), or treated with Synthroid, levothyroxine, Eltroxin and other T4-only meds (which leaves us hypothyroid to our own degree and kind), no wonder we, as informed patients, started seeing heart problems crop up in each other!
Why do our hearts suffer?
The answer for many appears to be from low levels of T3 (Triiodothyronine), the active thyroid hormone. Your heart’s health and your entire cardiovascular system is highly dependent on adequate levels of T3 for its well-being. T3 improves contraction and thus cardiac output, for one. So if it’s low, output goes down.
T3 keeps your metabolism running well, which helps clear out excess arterial fatty deposits. So if its low, cholesterol and fatty acids go up.
Or if you can understand a biological explanation of what T3 does for your heart: “Bioactive T3 is a powerful regulator of inotropic and lusitropic properties of the heart through their effects on myosin isoforms and calcium handling proteins in particular.” (http://circ.ahajournals.org/content/122/4/385.long)
A good explanation of what poor levels of T3 can do to the heart comes from this article:
…the heart is particularly vulnerable to reductions in biologically active T3 in plasma because cardiomyocytes have a negligible capability to generate T3 from locally converted precursor T4. Consequently, when circulating T3 is low, the myocardium may become relatively hypothyroid.
But my doctor says T3 is dangerous for my heart!
They are stupidly saying that because of the way T3 will reveal a CORTISOL problem with hyper-like symptoms, including a higher heartrate or palps. T3 can even reveal low aldosterone, another adrenal steroid. Again, it’s not the T3 that’s the problem: it’s what it’s REVEALING that is the problem.
When starting on or raising T3 in the presence of EITHER high cortisol, low cortisol, a mix of both, or low aldosterone, you can find yourself with hyper-like symptoms and a higher heartrate or palps. That’s because the wrong amount of cortisol, or low aldosterone, causes T3 to go high in the blood, and we call that pooling.
And IRONICALLY, do you know WHY we get a cortisol or aldosterone problem and pooling?? From being on nothing but T4, or being held hostage to the TSH which underdoses us. Our doctors are often causing this problem!!
***This is where we have to order and do a saliva cortisol test to see what our cortisol problem is. This isn’t about blood cortisol. And read about aldosterone, as low levels can also cause problems that T3 will reveal.
We should always, always have T3 in our treatment from the beginning of having hypothyroid treatment!
There are NUMEROUS medical studies which underscore that the judicious use of T3 (and can apply to NDT when used correctly since it has direct T3) has been very positive for heart and cardiovascular health. For example, this study states the following:
Clinical studies have shown that mild forms of thyroid dysfunction, both primary (subclinical hypothyroidism and subclinical hyperthyroidism) and secondary (low T(3) syndrome) have negative prognostic impact in patients with heart failure. In these patients, the administration of synthetic triiodothyronine (T(3)) was well tolerated and induced significant improvement in cardiac function without increased heart rate and metabolic demand.
Another study found positive results with T3, stating: Altogether, our data indicate that short-term administration of substitutive doses of synthetic L-T3 state reduces activation of the neuroendocrine system and improves LV SV in patients with ventricular dysfunction and low-T3 syndrome.
This study reveals that T3 plays a key role in repairing a damaged heart: The potential of TH (thyroid hormones) to regenerate a diseased heart has now been tested in patients with acute myocardial infarction in a phase II, randomized, double blind, placebo-controlled study (the THiRST study).
In fact, research has shown that low T3 can mean a negative outcome in cardiac patients: …low T3 concentrations are a strong independent predictive marker of poor prognosis in cardiac patients and might represent a determinant factor directly implicated in the evolution and prognosis of these patients.
Here’s a study that shows that even low dose T3 can help even with hypertension in improving the diastolic: While cardiac dysfunction could not be completely prevented in the absence of antihypertensive treatment, T3 may offer additional benefits as an adjunct therapy with possible improvement in diastolic function.
And the above is only a smattering of all the medical studies about the importance of T3 for one’s heart
Seven reasons for a high heartrate (with #1 in the below graphic should also be low aldosterone):
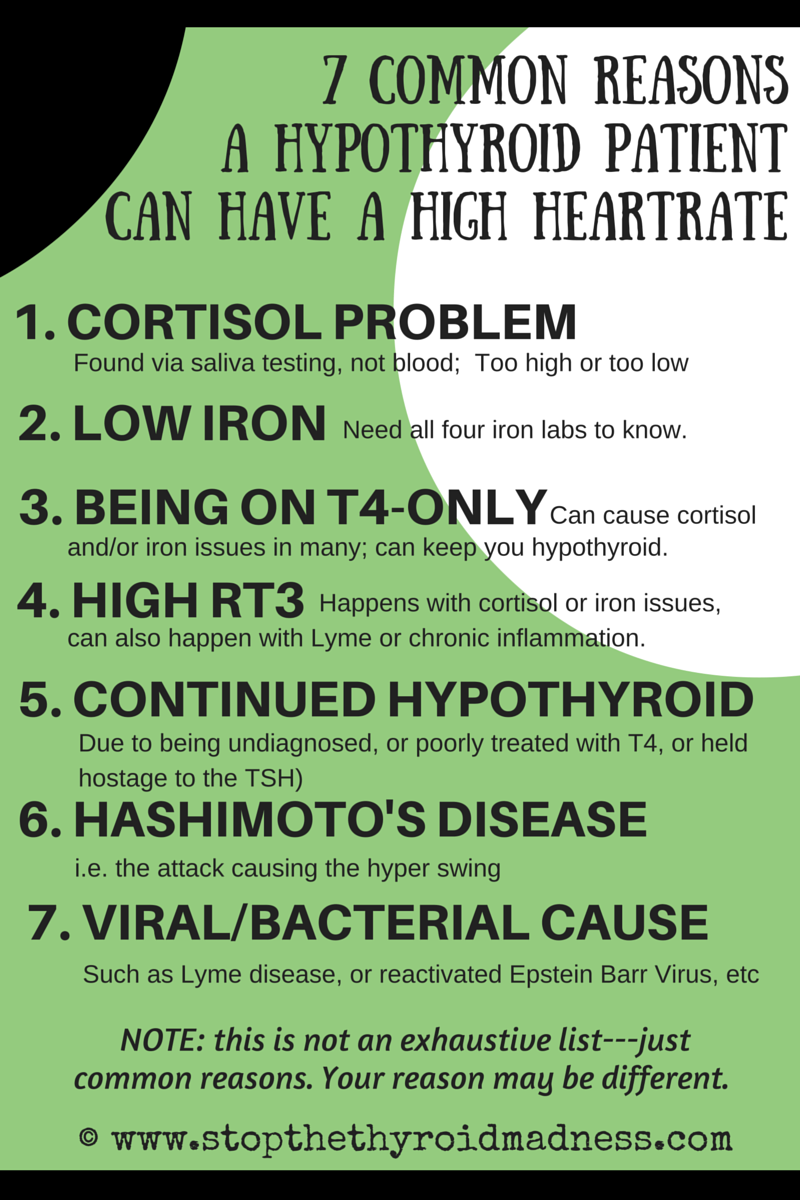
Summary of graphic. Seven reasons for having a heart problem for a lot of thyroid patients include a cortisol problem, having inadequate levels of iron, being on T4-only like Synthroid or Levo, having a high reverse T3 (RT3), being undiagnosed hypothyroid or held hostage to the TSH lab test, Hashimoto’s, or Lyme, EBV, etc.
What about the A-fibrillation I was diagnosed with?
FYI: Atrial fibrillation means your heart’s two upper chambers will beat irregularly and you might feel a sudden pounding or racing of your heart. It will cause poor blood flow, meaning you could feel tired and weak as a result. It can also cause heart palpitations. (Not all heart palpitations are the result of A-fib, by the way. A few examples: low potassium levels can do it, stress can do it, mitral valve prolapse can do it, etc.
Danish researchers found that even mild hyperthyroidism can increase your risk of having atrial fibrillation. And with Hashimotos driving you into a hyper state, plus some patients having both antibodies to Hashi’s and Graves disease, it might be related to A-fib in some patients.
Another presentation titled Atrial Fibrillation in Hypothyroidism found that hypothyroidism itself can lead to A-fib.
A 2009 study found that subclinical hypothyroidism might increase the risk of transient atrial fibrillation.
Bottom line, no matter what the cause…and there can be different causes…A-fib has serious consequences if it’s not addressed upfront, so work with your doctor. And with any treatment your doctor finds for your A-fib, patient experiences show us that being on the right thyroid treatment (which too many patients found is not T4-only), and treating any cortisol or iron issues before raising, may also be key to avoiding A-fib.
One word of caution…
I, Janie, have Mitral Valve Prolapse (MVP). That means the mitral valve on my heart is very sensitive. And before I started on NDT, I would get palpitations here or there in response to stress or activity. So when I started on NDT, I got a lot of palps. And with each raise, I got palps. But they always subsided within 5 days after each raise, and went away. And we have all learned to start on smaller amounts of NDT (like one grain) and raise in smaller amounts (like 1/2 grain) to allow our T3-starved hearts time to adjust to this wonderful and powerful hormone. Today, I RARELY get palps anymore as compared to those I got before I got on NDT, so my experience confirms that T3 in my treatment made a huge difference in my heart!
Bottom line, as you switch to NDT, or use T3-only in your treatment, work with your doctor while teaching him about the efficacy of T3 to your heart! And don’t forget to do a saliva test to see if you already have a cortisol problem or low aldosterone that needs treatment, and which T3 will reveal via hyperlike symptoms as you raise.
Come on over the STTM Facebook page and “Like” it for daily inspiration and information!
Important note: STTM is an information-only site based on what many patients worldwide have reported in their treatment and wisdom over the years. This is not to be taken as personal medical advice, nor to replace a relationship with your doctor. By reading this information-only website, you take full responsibility for what you choose to do with this website's information or outcomes. See the Disclaimer and Terms of Use.