Have you gotten a diagnosis of Hashimoto’s disease? Or suspect it? It’s a common cause of hypothyroidism due to an attack on your thyroid by your confused antibodies. You also might see it called thyroiditis. And Hashi’s has its own issues that one without it may not have. So start with this informational page to become more informed!~Janie, hypothyroid patient and site creator
Hashimoto’s disease, aka Hashi’s, is an autoimmune attack on one’s thyroid and based on a dysfunctional immune system, i.e. your thyroid is being attacked by your immune system via antibodies it releases (blood proteins), attempting to destroy your gland as if it’s some vile enemy. Hashi’s may be the most common thyroid disease, especially with women, but probably not quite s high as 90% as some claim, but still a high percentage.
How do I know that Hashimoto’s has begun it’s dirty deed in me?
Hashi’s may start out silently which can last years. The Stages of Hashimoto’s disease as mentioned by patients are examined in the book Hashimoto’s: Taming the Beast by Janie Bowthorpe.
But the attack will eventually show itself, causing inflammation and gradual destruction of your thyroid gland with miserable side effects to match. It can also cause nodules or swelling in some individuals.
Dr. Alexander Haskell once proposed another reason for Hashi’s: that the thyroid first becomes inflamed due to being hypo and the excess production of the TSH, which then leads to Hashimoto’s in those susceptible. But check out all sorts of causes in the book Hashimoto’s: Taming the Beast.
Chapter 2, Part 2, Gut health in the book Hashimoto’s: Taming the Beast
What issues can make this worse?
Hashimoto’s disease can be made worse by gut issues, whether poor levels of good bacteria, Small Intestinal Bacterial Overgrowth or Dybiosis, allergies to foods, reactions to any foods, and more. They need to be addressed. There are two chapters about gut health problems in the book Hashimoto’s: Taming the Beast.
How do I confirm Hashimoto’s via labs?
Hashi’s is usually confirmed by two antibodies labs, and you need both, not just one:
anti-TPO
TgAb
The first antibody, anti-TPO, attacks an enzyme normally found in your thyroid gland, called the Thyroid Peroxidase, which is important in the production of thyroid hormones. The second antibody, TgAb, attacks the key protein in the thyroid gland, the thyroglobulin, which is essential in the production of the T4 and T3 thyroid hormones.
Note: it is unfortunately common for a doctor to only do ONE test, which could look fine, yet the one your doctor didn’t order reveals Hashi’s. Thus, we as informed patients know we need BOTH tests. Also, if your doctor just chooses the TPO, there are other autoimmune diseases that can cause a rising TPO.
I suspect I have Hashimoto’s, but my antibodies aren’t showing it?
That’s called Seronegative Hashimoto’s. Many doctors do an ultrasound to confirm it, as they will see a particular pattern on your thyroid from the attack. For more difficult-to-discern cases, doctors might do an FNA test (fine needle aspiration). They will look for “Hurthle Cells”, large granulated cells, which are associated with Hashimoto’s. But for most, an ultrasound works well.
What if my test results show “some” antibodies, but in the “less than” or “normal range??
Having some antibodies in that normal range is, in fact, perfectly normal. Don’t let someone falsely tell you that you have to have zero antibodies. Why would we have “some”? Because one function of the immune system is to use antibodies in the removal of dead cells.
One exception is if your “normal” antibodies are creeping up in that range towards the top end. That might mean it’s time to practice good offensive strategies, like taking care of your gut health, avoiding foods you react to, treating any inflammation, moderating stress in your life, getting the right amount of sleep. Find “supportive” immune system supplements. Many of those normal or less-than results do not move up to having full-blown Hashi’s when patients take care of themselves.
Want to order your own labwork to discern if you have Hashi’s?? STTM has partnered with key lab facilities, creating the right ones just for you to discuss with your doctor. No prescription needed! Go here: recommended labwork
What are symptoms of autoimmune Hashimoto’s?
Hashimoto’s symtoms graphic
Summary of graphic: Symptoms of Hashi’s can include poor stamina, easy fatigue, depression, feeling cold, gaining weight, dry skin or hair, lowering of voice and constipation. But it can also cause diarrhea, anxiety or panic, fidgetiness, feeling hot or cold, tightness in throat, inflammation, and thyroid nodules. You can be hyper-like one time, and hypo-like another time.
Why is it important to know if I have full blown Hashi’s?
As Hashimoto’s increases, you will tend to swing between hypo and hyper, making dosing by labs, and especially the TSH, impossible. Your labs will be high one time, and low the next–back and forth–causing some doctors to falsely proclaim you have a mental health “Bi-polar” condition.
In reality, the hyper is caused by the release of thyroid hormones into your blood due to the destruction, or as an Australian patient calls it, the “yeeha” of her swing. The hypo is caused by the lessening function of your thyroid due to the attack.
Is it a good idea just to “watch it” as my doctor wants to do?
“Watching” your Hashi’s is akin to watching a dog chew off your leg. It can not only last for years, but cause all sorts of problems along the way of its destruction. Those problems include adrenal stress or the pairing with other autoimmune problems like Celiac disease, and more. And once you add adrenal problems to the mix, you’ve got more issues to tackle. Instead, why not just stop the attack and all the consequences, as explained below. Makes a whole lot more sense, says a patient who suffered through what she calls the “insane watching”. This is one of many areas that is covered well in the book Hashimoto’s: Taming the Beast.
Are there some foods I should NOT eat with Hashimoto’s?
Yes, and they can include foods with gluten, nightshades, sugar, dairy and more. Find out if YOU react to certain foods. Many do, but not all.
There is EXCELLENT info about foods, how Hashi’s patients have reacted to them, how to eat differently, in the book Hashimoto’s: Taming the Beast.
What are particular diet plans to help against inflammation and the rise of antibodies?
Learn about eating Paleo. The stricter form is called AIP, which stands for Autoimmune Paleo. There are many websites about it…here’s one. Less strict than AIP is just called the Paleo way of eating. It’s based on the idea of what “cavemen” would have eaten. Again, many websites about this, and here is one. Author Elle Russ has an excellent book about it.
Do I treat my Hashimoto’s with thyroid meds?
Because Hashimoto’s means a nutty attack on the thyroid, most end up with hypothyroidism. So the majority of Hashimoto’s patients still end up needing thyroid medications to treat their hypothyroid state.
And patients have learned that the best way is with T3 in your treatment, first and foremost, such as T4/T3. Some who have a high RT3 (reverse T3) end up with T3-only. Here’s all about the use of T3.
The RIGHT TREATMENT, which isn’t T4-only, can help Hashi’s patients see the attack cease just from treatment alone, probably due to improvement of the immune system. Every cell in your immune function needs T3! Some doctors have unwisely recommended non-treatment until labwork “stabilizes”, but that could take months and years, and you continue to suffer.
WHOOPS…to successfully raise meds with T3, we have to have good amounts of iron and cortisol!! If you have bad reactions, it’s due to problems with either, NOT the medication in the vast majority of cases. Study: https://stopthethyroidmadness.com/ndt-doesnt-work-for-me
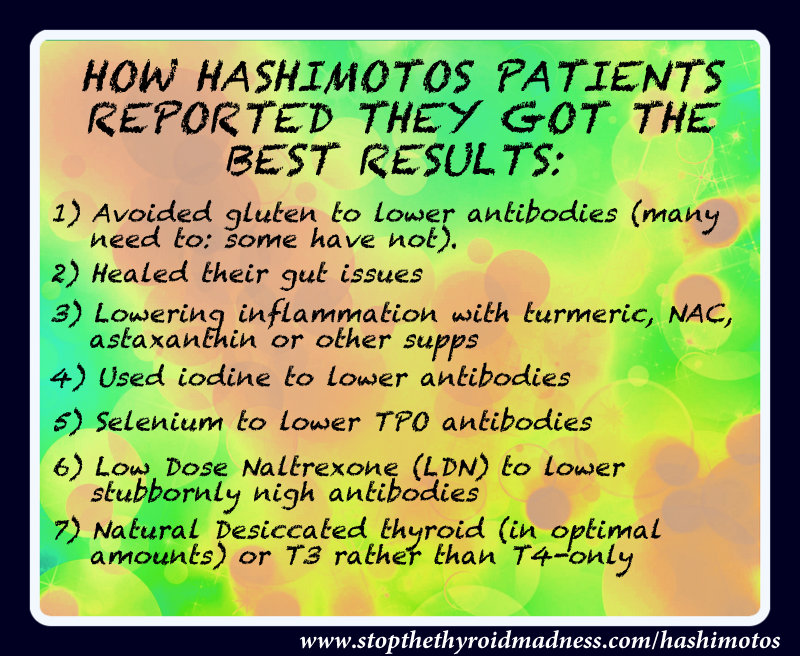
Many patients have reported that selenium supplementation, up to 400 mcg, has helped, especially if you have high anti-TPO. (But do check your selenium labs first to make sure it’s not too high) Some patients have also reported that iodine supplementation outright lowered their antibodies–yes, you read that right, contrary to some who tell you no iodine. Low Dose Naltrexone has helped the more stubborn cases. See below. And of course, you have to take care of any gut problems!
For the inflammation caused by Hashi’s, patients might use good supplements like Curcumin, Ginger, NAC and more.
But my antibodies are going up with T3 in my treatment…
Of course they will! Your body’s immune system is confused and thinks thyroid hormones are the enemy. But as patients persisted in raising to find their optimal dose, that rise stopped, and antibodies even fall for many! See the second section below. Those who have STUBBORN antibodies either use LDN.
I keep reading that we shouldn’t be on a working natural desiccated thyroid (NDT) if we have Hashi’s. Is that true?
No, not according to a huge body of Hashi’s patients who reported they have soared with a working NDT. Granted, patients have noticed that if they stayed on lower doses too long and/or didn’t raise high enough, quick enough, it fed the attack, not stopped it. You then have further swelling in your throat, or hair loss, or high anxiety, or a raise in your antibodies…and heightened hypo symptoms with a higher TSH. And doctors who aren’t knowledgeable about desiccated thyroid might put you back on synthetics, or take you off your meds completely. The solution discovered by patients is to raise the desiccated thyroid faster and according to the elimination of symptoms and NOT labs. Many seem to end up in the 2-5 grains area to stop that attack. This is where individuality comes in.
A caveat: 2020 saw three US brands recalled after patients had been complaining of seeing their hypo symptoms coming back. They were Naturethroid, WP Thyroid, and NP Thyroid. Armour continued to work. And many patients just switched to T4 and T3 and worked to get their frees optimal.
I am swinging between hypo and hyper, and my doctor says I shouldn’t be on thyroid meds when I’m hyper. Is that correct?
The hyper when you have Hashi’s is caused by the die-off of thyroid hormones from the attack and their dump in to your blood. You also will swing between hypo and hyper as explained above. But to say you shouldn’t be on thyroid meds is wrong according to the vast experience of Hashimoto’s patients. Being optimal on thyroid meds like natural desiccate thyroid or T4/T3 improves the immune system and often stops the attack. You’ll have to fight your doctor’s tendency to hold you too long on each raise, or to dose you by the TSH or other labs.
Are there exceptions to the latter?? Yes, there are always exceptions, and someone may find the need to back off thyroid meds until they get past the thyroid hyper of Hashi’s.
What about Low Dose Naltrexone and Hashi’s?
Naltrexone is a an opioid antagonist, and when taken in low doses, has been found to elevate your endorphins, which in turn promotes better immune function. Thus, many Hashi’s patients report a lowering of their antibodies while using this medication. It may be challenging to get a prescription from your doctor if he or she hasn’t learned about the effectiveness of LDN, so you can refer him to this LDN science site.
A WAY TO MAKE YOUR OWN: The way it’s used by patients is to dissolve one 50 mg tablet with 50 ml of distilled water in an amber glass bottle. It has to be shaken before use. Using a baby medicine dropper, or even more accurate, a syringe, many patients start at 1.5 ml and mix it with water or juice. It’s taken a bedtime, since the best action occurs during sleep. Patients report vivid dreaming the first several nights, but it goes away. They slowly make their way up to 3 mg. The maximum is 4.5, but many like the results from 3 mg. Once antibodies fall, you may suddenly find yourself on too much medication for your needs. Check into LDN groups Facebook. Read more here.
Is there a connection between pregnancy and Hashi’s?
Pregnancy can be a strong precursor to developing Hashi’s, since the increased activity of your immune system can either worsen an autoimmune disease you already have, such as thyroiditis, or cause it to appear.
Can I take iodine when I have Hashi’s?
Yes!!! If you hear or read someone state that all Hashi’s patients should avoid iodine, you might want to question other things you hear or read from that source. Because there are a strong body of Hashi’s patients who report doing quite well on iodine, and some outright report that it was their iodine use that lowered antibodies, even if others need extra help. Doing an iodine loading test can confirm if you have low iodine. And since iodine is the main component of thyroid hormones, plus has anti-cancer benefit, the use of iodine can be a wise decision.
For others, it’s trickier, since iodine can promote the detoxification of certain toxins like bromide, and this can exacerbate symptoms. And they wrongly blame the iodine, when it’s the detox causing issues. This is why it’s important to learn about companion nutrients to counter the die off. Bottom line, we let each person decide what is right for them.
Don’t guess if you have either too low or too high cortisol. Order a saliva cortisol test and find out what is going on.Then compare your results to this page, NOT just the graphic they provide afterwards.
What if I have BOTH antibodies for Hashi’s and Graves?
It’s called Hashitoxicosis.
This is a more difficult form of a thyroid autoimmune condition where you can have Hashimoto’s antibodies, PLUS an elevated TSI (Thyroid Stimulating Immunoglobulins)–the latter which is a member of the Thyroid Stimulating Hormone Receptor Antibody (TRAb) family, and which at least 80% of Graves patients can have. You can both hyper and hypo symptoms. Low Dose Naltrexone has been helpful for many individuals who have these antibodies.
Bottom line?
Every Hashimoto’s patient should take the time to study the patient-to-patient book Hashimoto’s: Taming the Beast. Note the “patient-to-patient”—it’s also full of important patient-to-patient experiences and wisdom to help you TAME THE BEAST! You can read more here: https://stopthethyroidmadness.com/hashimotos-taming-the-beast
Interesting side note: Both Hashi’s and Graves disease (hyperthyroidism) can have elevated anti-TPO. “The frequency of elevated anti-TPO levels in patients with active autoimmune thyroiditis was 90% (clinical diagnosis Hashimoto thyroiditis) compared to 64% in patients with overt hyperthyroidism (clinical diagnosis Graves’ disease).” Pub Med article here.
(Important note: STTM is an information-only site based on what many patients have reported or learned in their treatment. Please work with your doctor. This is not meant to replace that relationship or guidance, and you agree to that by reading this website. See the Disclaimer.)
Important notes: All the information on this website is copyrighted. STTM is an information-only site based on what many patients worldwide have reported in their treatment and wisdom over the years. This is not to be taken as personal medical advice, nor to replace a relationship with your doctor. By reading this information-only website, you take full responsibility for what you choose to do with the information on STTM or its outcomes. See the Disclaimer and Terms of Use.
 Are there some foods I should NOT eat with Hashimoto’s?
Are there some foods I should NOT eat with Hashimoto’s?  Are there some foods I should NOT eat with Hashimoto’s?
Are there some foods I should NOT eat with Hashimoto’s?