Optimal Lab Values–how we as patients learned to interpret lab results
Years ago in a group started by me, (which ultimately started the Stop the Thyroid Madness movement, we began to notice that healthy people / healthy levels were falling in a certain “part” of the range, not just anywhere in the so-called “normal” range. That was huge information. Check out below. ~Janie, hypothyroid, late-onset Hashi’s patient and site creator
Fair Warning: This information is copyrighted. That means if you use it anywhere without the permission of the owner, in addition to failing to state where it’s from even after getting permission, you are doing it illegally and are making yourself open for definitive legal action.
By the way: How we learned to prepare for labs
For most of the below, we stay off what we are testing for a minimum of 12 hours, and only take meds or supps after the blood test.
For iron, we learned to be off for “up to” 5 days (based on the Iron Institute), i.e. to see what we are “holding onto”. But a few days is fine.
For salivacortisol,we learned to be off any cortisol-containing or cortisol-changing supplement for at least one week. But work with your doctor. See the list here. There may be some things you canNOT get off without having problems, so it will slight effect your results.
For thyroid labs, we take our thyroid meds the day before as usual (except bringing a nighttime dose to the afternoon or early evening), THEN we test first thing the next morning BEFORE taking thyroid meds for that day. And it’s NOT about a rigid set of hours as many are falsely telling you.
THYROID RELATED
Free T3 (Free Triodothyronine):
Those without a thyroid problem: several points above mid-range. The exception: if you are on NDT, and the free T3 is above mid-range, plus the free T4 is low in the range—the latter free T3 might represent pooling–going high in the blood and not making it to the cells due to stressed adrenals.
Those who are optimal on NDT or T4/T3 will see a free T3 in the very top numbers of the range, ALONG WITH a mid-range or slightly above free T4.
Those who are optimal T3-only usually see a free T3 in the top numbers (occasionally very slightly over the top).
A high free T3 with a low free T4 while on NDT or T4/T3: pooling
Free T4 (Free Thyroxin/Thyroxine):
Generally, those without a thyroid problem have a free T4 just slightly above mid-range. This will go with a free T3 above where that free T4 falls. There can be slight exceptions
Those who are optimal on NDT or T4/T3 will tend to have a free T4 around MID-range along with a free T3 towards the TOP part of the range.
If on nothing but T3 and optimal at the top number of the range, Free T4 will be low.
FT4 can start rising when RT3 is going up, then can fall.
RT3 (reverse T3, the inactive hormone)
Those without an RT3 problem seem to be in the bottom 2-3 numbers of any range. Some are even below range with no issue. Higher and RT3 is going too high, making you more hypo.
TSH (thyroid stimulating hormone)
Sadly, it can look great while you have raging hypothyroidism; or it can be high while you have hypothyroidism, meaning your hypo has gone on awhile. Thus, we only use it to discern hypopituitary when on no meds: a low TSH with a low Free T3.
It is normal to see your TSH fall, be low in the provided range, if not below, when you have T3 in your treatment, and that is NOT hyperthyroidism, and does NOT mean to lower your meds.
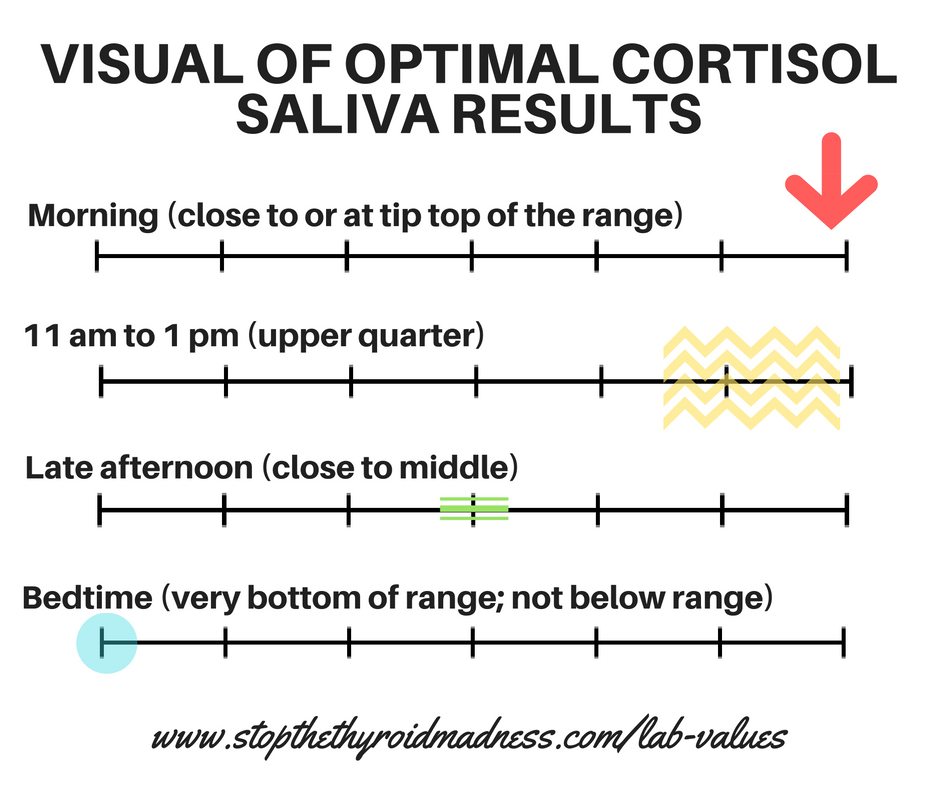
Here are the consistent results of people who do not have an adrenal problem, which is also your target when on HC/hydrocortisone:
8 am(or when you normally wake up): at the tip top part of the range (if top of range is 9.5, people are right there, or 9.4, 9.3 at the lowest.
11 am-noon (or approx. 4 hours after you woke up): in the upper “quarter”, closer to the bottom of that upper quarter
4-5 pm (or approx. 4-5 hours after the above): right “around” mid-range
Bedtime: at the very bottom (Literally. So if range is 1-4, people are at 1, not even 2)
And here’s where to order your saliva cortisol testhere through STTM.
ALDOSTERONE
In most ranges, people are falling significantly above mid-range (and close to the top) who do NOT have an aldosterone problem or low aldosterone symptoms. If they DO have an aldosterone problem, they are midrange or lower.
HASHIMOTO’S RELATED
TbAb (Anti-thyroglobulin):
If the result is below the “less than” mark, or in the range provided, you may be fine, but you need to do the anti-TPO shown below, as well. If above range, Hashimoto’s.
Anti-Tpo (anti thyroid peroxidase):
In the range seems fine. If this is above the range, you’ve got the autoimmune thyroid disease Hashi’s.
LIVER RELATED
ALT (alanine transaminase) is an enzyme released by the liver. We have noticed repeatedly that healthy people/healthy livers usually fall in the teens of most ranges. It seems more accurate that the AST, as well. .
IRON RELATED
Women when optimal (note that “~” means approximately):
Iron: ~110 (or 23ish in ranges that go up to 27 such as in the UK)
% Sat: ‘close’ to 34 or35% (or .34 / .35)
TIBC: ~low 300’s
Ferritin: 50’s or higher (optimal 70-90) (if it’s much higher, it’s about inflammation.
Iron: upper ~130’s (or upper part of range in Canadian or European ranges that go up to 30ish)
% Sat: ~38% or higher (or .38 in above ranges)
TIBC: ~low 300’s, sometimes lower
Ferritin: 110ish
P.S. #1. If serum iron, % saturation and ferritin (all three) are high, you may have the genetic hemochromatosis and you can ask your doctor for testing.
P.S #2. If TIBC is midrange or higher with high iron, you’ve got a methylation problem.
MISCELLANOUS B12:
Upper quarter of the range. The urine test Urinary Methylmalonic Acid, also called the UMMA, can be added since it is a very sensitive detection and if high, will reveal a true B12 deficiency.
FEMALE HORMONES:
Scroll down to NOTES below.
FOLATE:
Standard range is 3-17, so optimal would be at least the top third of that, we have noted. Higher for MTHFR.
RBC MAGNESIUM:
Mid-range or higher
SELENIUM:
Selenium should never be above the range. If slightly over the top, it appears to be on too much. If much more than slightly over, you may have a methylation problem.
SODIUM: (“close to” 142)
Sodium can occasionally be a point or two less. Should not be in the 130’s anywhere, we have noticed in healthy people.
POTASSIUM: (~4.8 when the range goes up to 5.2) That’s where we see it a lot in healthy individuals.
Serum potassium is above. RBC Potassium is in the 70-95% of the range. Tell the lab tech NOT to use the tourniquet for drawing blood. It can falsely raise your potassium result.
RENIN:
If renin is high in the range along with a low aldosterone, you have an adrenal cause. If both hormones are low in the range, you ‘may’ a pituitary problem. Always tested along with Aldosterone to see if your problem is due to the adrenals (primary adrenal insufficiency) or your pituitary (secondary adrenal insufficiency).
VITAMIN D (25-hydroxy):
50-80 is the most mentioned goal even though informed patients shoot for the 60-80 range, which is also recommended by cutting edge doctors.
A second Vitamin D test you can ask for: Vitamin D1, 25, the biologically active form of vitamin D. Why? You could have a genetic problem called the VDR mutation, i.e. the Vitamin D25 Receptor Mutation.
ZINC:
Top third of the range is optimal
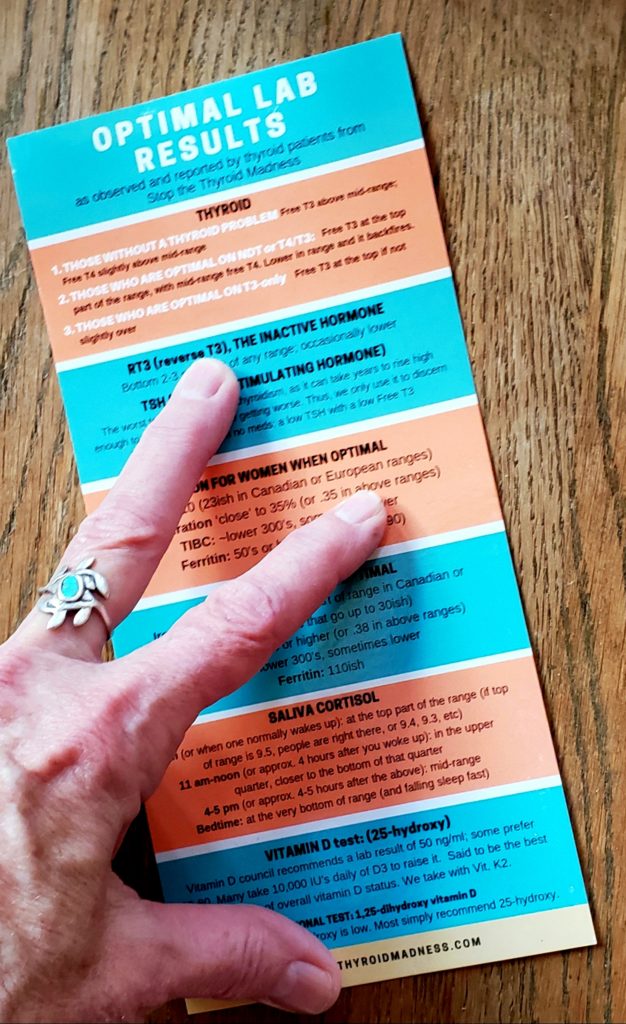
Hey, like convenience?? Consider getting the handy two sided, 4″x8″ Lab Values card for easier reference! You can also use it as a bookmark in your STTM books. Or place it in easy reach to review. Give these to your doctor, family members, and/or friends. THEY GET CHEAPER THE MORE YOU BUY. Go here and click on Lab Values card: https://laughinggrapepublishing.com
What about the newest fad of no ranges, and instead you just see “less than” or “greater than” goals? OR the same with the actual lab results?
Those are a pain in the rear, we as patients have noticed. So we’re forced to guess that if a ‘range” given is “<128” (just an example), the 128 could be the top of what would have been a range. Or if we get an actual lab result of “>128”, the 128 represents the bottom of the range. But we have no idea what the other end of the range would have been.
WANT TO ORDER YOUR OWN SALIVA CORTISOL TEST?? Go here.
NOTES ABOUT IT ALL:
THYROID RELATED
FREE T3 (may also say Free Triiodothyronine–free in front is measuring what is unbound and available)
This is the ACTIVE hormone–the thyroid hormone that changes lives, removes depression, keeps metabolism up, keeps cholesterol down in most, removes aches and pain due to hypo, keeps bones healthy, keeps heart healthy, keeps liver healthy, on…and on…and on.
What if your free T3 is super high with continuing symptoms, and/or a lower free T4? That’s called pooling of the T3, and can be a clue you have a low cortisol issue. If not on thyroid medication: 1) If your free T3 is high, you could have Hashimoto’s disease, which will need the two antibodies tests to discern it, or Graves disease, which needs the TSI test. 2) if your free T3 is mid-range or lower, and in the presence of hypothyroid symptoms, you may have hypothyroidism, no matter how low the TSH. Patients find it’s not a good idea to take any T3-containing product on the morning of a test. Work with your doctor.
FREE T4 (may also say Free Thyroxine–having free in front is measuring what is unbound and available.)
T4 is the thyroid storage hormone. It’s meant to convert to the active thyroid hormone T3 and that’s a good thing when it’s going on behind the scene. But we learned the hard way that the body is NOT meant to live for T4 ALONE in our treatment.
REVERSE T3 (RT3):
This is the inactive hormone. In us, whether Hashimoto’s or non-autoimmune hypothyroid, it will usually go up with low iron, inflammation, or high cortisol. It can also go up due to a viral infection like the flu or related, a physical injury, when detoxing high heavy metals, Lyme disease, mold illness, a tooth infection, after surgery, etc. (See the revised STTM book for further details.)
TSH:
The worst test to go by. Why? TSH stands for Thyroid Stimulation Hormone. It’s a messenger hormone released by the pituitary gland to tell the thyroid to produce more hormones when needed. So theoretically, the higher the TSH lab test, the more your body is screaming at your thyroid to produce! produce! Creators of the TSH lab test came up with a ‘range’ that supposedly corresponds with healthy thyroid function. So theoretically, if your TSH lab results are higher than the range, it would imply something is triggering your actual TSH to be a little too active in screaming at your thyroid. That something would be a diseased thyroid, called hypothyroid.
But there are problems with this method of diagnosis. First, you can have a so-called normal result, yet be clearly hypothyroid with symptoms. Why? Because the TSH test cannot measure if all your cells & tissue are receiving the released thyroid hormones. Some may be (thus the normal TSH result) and some may not be (thus your clear symptoms).
Second, if you have Hashimoto’s, your lab results can swing between hypo and hyper, & your lab test may be representing the middle of the swing.Better to diagnose and dose by is the free T3 and free T4, NOT the TSH.
Is it ever useful? We have noticed that the best way to use the TSH lab test is in diagnosing a pituitary problem, not a thyroid problem. A very low TSH with a low free T3 gives away a hypopituitary issue. Otherwise, unlike extremely clueless doctors, we honestly pay no attention to it.
T7, TOTAL T3 (no free in front), TOTAL T4 (no free in front), UPTAKE, etc:useless and outdated for our particular needs….
ADRENAL RELATED
24-HOUR SALIVA CORTISOL Saliva testing is an at-home test to evaluate your circadian and cellular cortisol levels at key times during a 24 hour period. It’s more accurate than blood cortisol, we saw repeatedly, since the latter measures both bound and unbound cortisol, not cellular levels like saliva, and thus blood can give a false idea of what is really going on. You can look low, yet be high; you can look high, but be low. It’s crazy
Note: we learned the hard way that it’s impossible to know what is going on if you use a lab facility like Quest that has the range as “less than” or “more than” a number. (i.e. < or >). More problematic saliva tests mentioned on the Recommended Labwork page.
ALDOSTERONE: This test measures the adrenal hormone aldosterone which helps regulate levels of sodium and potassium in your body–i.e. it helps you retain needed salt, which in turn helps control your blood pressure, the distribution of fluids in the body, and the balance of electrolytes in your blood. Symptoms of having low aldosterone range from craving salt, low sodium blood test, peeing more or sweating more, blood pressure issues. You can have one more or more. This is best tested in the morning and with no salt intake for 24 hours. Women need to do it in the first week after their period, since rising progesterone can also raise your aldosterone. Testing should not be done with severe illness (aldosterone falls in response to severe illness), during periods of intense stress (aldosterone rises), or right after strenuous exercise (aldosterone rises). Being pregnant can result in doubled amounts of aldosterone.
DHEA: This is the mother all steroid and sex hormones. Healthy adults are at their highest levels in young adulthood and begins a general decline by your 30’s, and is the lowest level as you become older, such as the 60’s and up.
ACTH STIM (not needed for most, we’ve noted, unless there is suspicion of a serious adrenal problem like Addison’s disease):
The ACTH Stimulation test, also called the Cosyntropin test, measures the ability of your adrenals to be stimulated by the ACTH, a pituitary hormone, and is used to diagnose Addison’s or Cushing’s disease, as well as hypopituitary. Usually done in an out-patient setting and takes only a few hours. A synthetic ACTH is injected into your arm and the response of your plasma cortisol levels are measured. You’ll need to fast, and the test is usually done in the morning. You cannot be on any cortisol medications or supplements. An ACTH plasma test is often done at the same time to measure the amount of ACTH being secreted by the pituitary gland. Your cortisol levels will double if your adrenals are not diseased. The ACTH has not been found to be a good test for the kind of adrenal fatigue manifested by thyroid patients, which is sluggishness, not disease.
HASHIMOTO’S RELATED—two antibodies at the minimum
TgAb (Anti-thyroglobulin)measures the level of the antibody protein anti-thyroglobulin in order to discern the presence of Hashimoto’s disease. (No, we have not observed that it has to be zero to be free of having Hashi’s!. Anywhere in the provided range is normal and fine.)
Anti-TPO (anti Thyroid Peroxidase) measures the thyroid antibody TPO. TPO refers to the enzyme made in your thyroid gland which helps produce thyroid hormones.
IMPORTANT NOTE: since some with Hashi’s can also have the Graves antibodies, many patients are also testing both TSI (Thyroid-Stimulating Immunoglobulin) and TRAB. (Thyrotropin receptor antibodies). TSI 80 or below is considered remission. Ideally, you should have zero TSI. Labs use either >140 or >125 (depends on the lab) as positive for Graves Disease. TrAb should be “undetectable”. Remission is when TrAb (PLUS the above TSI under 80) is less than .9. They also use a test called the TBII but we’re not sure what the perfect levels are for that one yet.
A very small body can show no antibodies, yet symptoms of Hashi’s. They need to talk to their doctor about an ultrasound.
Have Hashi’s?Highly recommended is the patient-to-patient book Hashimoto’s: Taming the Beast. Written in a concise style, avoiding long stories and chit chat for those with brain fog. Covers important details, also with four important patient-to-patient chapters, including one with 96 short testimonies on how actual Hashi’s patients got their antibodies down, and so much more.
IRON RELATED (and you need all four, NOT just ferritin. Ferritin is simply measuring storage iron)
SERUM IRON (also called just Iron or Total iron): This is measuring the amount of circulating iron that is bound to transferrin and serum ferritin. This is also what you treat. Unlike what you may read, we do NOT treat low ferritin. Big mistake.
PERCENT % SATURATION of IRON: Measures your serum iron divided by your TIBC. Reveals how much serum iron is bound by protein.
TIBC (Total iron binding capacity): Indirect measure of whether a protein called transferrin, produced by the liver, is enough to carry iron in the blood. NOTE we do NOT treat the TIBC. We treat the iron and % Sat. The TIBC just gives us interesting information as explained.
FERRITIN: Measures your levels of storage iron. a) If ferritin is high with lower iron, it’s about inflammation. b) If BOTH ferritin and iron are low, it’s simply low iron and the serum iron is to be treated, NOT the low ferritin. c) If ferritin is low and iron is good or high, that’s a methylation issue. AGAIN, WE DO NOT TREAT JUST FERRITIN as if we are treating iron.
In less common cases, higher ferritin can be from liver disease, alcoholism, diabetes, asthma, or some types of cancer. But for most of us, it’s just about inflammation from hypothyroidism, or gluten issues, or unknown. .
FEMALE HORMONES (serum is recommended over saliva)
***NOTE: Women with high SHBG can have slightly higher estradiol. i.e. when SHBG is high (>160 or so), some need a level of 150-160 blood to feel well. As a noncycling woman with higher SHBG, some might need a level of 50-80.
SHBG is mentioned because so many women on T3/NDT/testosterone treatment have high SHBG.
FSH and LH for cycling women should be 1:1 ratio. If LH is higher, that typically means PCOS. Labs must be taken day 2-4 of the cycle while bleeding.
FSH/LH <10 mIU/mL good/healthy egg reserve (nowhere close to meno—chance of conception, <3 excellent, 3-6 good, 6-9 fair)
FSH/LH 10-15 conception difficult but not impossible FSH/LH 15-20 perimenopause (probably not ovulating every month) FSH/LH 20-30 menopause almost certainly in progress (ovulation rare if at all regardless of bleeding) FSH/LH > 30 noncycling/postmenopause
Testosterone… both cycling and noncycling women
Free testosterone
2.10-3.20 pg/mL (US) serum
7.30-11.00 pmol/L (UK) serum
108-149 pmol/L (UK) saliva
36-47 pg/mL (US) saliva.
0.04-0.05 nmol/L serum
1.10-1.50 ng/dL serum
Total testosterone
28-38 ng/dL (US) serum
1.00-1.32 nmol/L (UK) serum
36-47 pg/mL (US) saliva
108-149 pmol/L (UK) saliva
SHBG… cycling and noncycling women (and men) 75-95 nmol/L
DHEAs (in the absence of adrenal fatigue or PCOS): Serum 175-225 ug/dL Saliva > 13ng/mL
OTHER
B-12: an essential vitamin also known as cobalamin. It’s water-soluble, meaning your body will excrete an excess. Wiki states it’s involved in the metabolism of every cell of the human body: it is a cofactor in DNA synthesis, and in both fatty acid and amino acid metabolism.
FOLATE: Also called B9, it’s important for prenatal development, as well as your blood cell health and methylation. Folate works with B12 in the use and creation of proteins. It’s “folate” thats needed instead of “folic acid”, especially if you have MTHFR. We don’t start too high, as for some of us, it can start the methylation process too strongly.
ALT AND AST: These measure the health of your liver–quite an important gland in your body involved in detoxing and more..
MAGNESIUM: This is an electrolyte mineral. See Janie’s blog post on magnesium.
SELENIUM:A powerful soil mineral that is stated to be anti-cancer. Also helps lower high TPO antibodies in Hashimoto’s patients.
SODIUM: An electrolyte which is outside cells, and has a balance with potassium, which is within cells. Sodium regulates bodily fluid and plays role in major bodily functions. This can be strongly related to whether you have low aldosterone or not.
POTASSIUM (can also be related to your aldosterone): Potassium is an electrolyte mineral which is within cells, and has a balance with sodium, which is outside cells. Potassium plays a role in healthy kidney, heart and nervous system function. When potassium is too high, it’s called hyperkalemia; when too low, hypokalemia. It can rise in the presence of low aldosterone (see above under Adrenals), then fall. Best to do an RBC potassium—red blood cell–which measures it in your cells.
Tell the lab tech NOT to use the tourniquet for drawing blood. It can falsely raise your potassium result.
Renin: An enzyme hormone that regulates the release of aldosterone and is done in conjunction with the aldosterone test. See this study. Always tested along with Aldosterone to see if your problem is due to the adrenals (primary adrenal insufficiency) or your pituitary (secondary adrenal insufficiency).
VITAMIN D test: (25-hydroxy): Vitamin D plays a huge role in your immune system and other important actions. Many thyroid patients are low in D due to digestive issues from being undiagnosed or undertreated, plus problems with Celiac or gluten intolerance.
When someone overreacts to Vit. D supplementation, it seems to point to a parathyroid problem.
ZINC:an essential trace mineral that promotes a good immune function. If this is too low, you risk seeing copper go up! Also important to test your RBC Zinc to see your cellular levels, because you have good-looking serum zinc and low RBC zinc! That happened to Janie Bowthorpe.
OTHER LAB RESULTS YOU MAY RECEIVE THROUGH YOUR DOCTOR:RED BLOOD CELL COUNT, HEMOGLOBIN (Hgb) HEMATOCRIT (HCT), MEAN CORPUSCULAR VOLUME (MCV), MEAN CORPUSCULAR HEMOGLOBIN (MCH), MEAN CORPUSCULAR HEMOGLOBIN CONCENTRATION (MCHC), PLATELET COUNT, RANDOM DISTRIBUTION OF WIDTH (RDW): Here is a great page explaining what they can mean: http://www.drkaslow.com/html/blood_cell_counts.html
CANADIAN LABS AND RANGES:
Serum Iron (range) Optimal results are usually in the mid-20’s for women, upper 20’s and higher for men)
Percent Saturation: same as US observations i.e. .35/35% for women is the ideal; .38/38% and often a little higher for men.
TIBC: when range is umol/L >45-77, low 60’s is noted when iron is looking good. If range is 50-70 umol/L, usually 1/4th above bottom of range.
Ferritin: range is often 15-200, and optimal for most women is 70-90, for men it’s 110-120.
Note: 60% of patients have a hematologic or neurologic response to B12 supplementation at a level <148 pmol/L
FOR THOSE WHO USE MATH—here’s how to find those “areas” of of lab ranges for thyroid, adrenals and TIBC
Top 1/4 of the range ** Math to do this, subtract the highest number in range from lowest number in range, divide by 4. Subtract this number to the highest number in range
Mid range ** Add lowest number in range to highest number in range. Divide by 2.
Bottom ¼ of the range: Subtract the right number of the range from the left number of the range, divide by 4. Add this number to the left number in the range
FOR THOSE WHO ARE VISUAL FOR THE ADRENAL CORTISOL SALIVA TEST:
Important notes: All the information on this website is copyrighted. STTM is an information-only site based on what many patients worldwide have reported in their treatment and wisdom over the years. This is not to be taken as personal medical advice, nor to replace a relationship with your doctor. By reading this information-only website, you take full responsibility for what you choose to do with the information on STTM or its outcomes. See the Disclaimer and Terms of Use.