TWO NEW BOOKS: Hashimoto’s: Taming the Beast & Updated Revision STTM book.
One of the most important steps we have to do, as hypothyroid patients no matter the cause, is to be INFORMED, which the Stop the Thyroid Madness books aka STTM books, provide you.
We have to look at the experiences and wisdom of patients before us who GOT WELL, which STTM gives you!
And we have to be prepared to guide our doctors with the information in the Stop the Thyroid Madness books…or fire them.
Why? Because 1) the medical profession simply doesn’t get it 2) their training is awful 3) they accept the dark-ages bad information they are fed without questioning.
Thyroid treatment should have NEVER been about…
- putting us on only one of five thyroid hormones like T4-only (backfires sooner or later with growing problems)
- the insane use of the TSH lab test and range for diagnosis or treatment (keeps us hypothyroid)
- falling anywhere in those ridiculous “normal” ranges (keeps us hypothyroid)
- “doing nothing” and “letting it run its course” for those with autoimmune Hashimoto’s (which increases inflammation and the risk of other autoimmune diseases)
And all the while we have had continuing problems, we are told…
You are normal
It’s not your thyroid
You need to eat less
You need to exercise more
You need to see a therapist
You need to be on an anti-depressant, or this med, or that med
PRESENTING…..
1) The “updated revision” of the world-renowned STOP THE THYROID MADNESS BOOK (info below)
2) HASHIMOTO’S: TAMING THE BEAST (a companion book to the above updated revision) See below.
About the updated revision STOP THE THYROID MADNESS: A Patient Revolution Against Decades of Inferior Thyroid Treatment, @2019
Same chapter titles. A continuation of former good info. Yet now, you have updates throughout the book.
- This world-renowned “bible of patient experiences” which is now updated, continues to have the life-changing information that it always has had with the same chapter titles…no matter your cause of hypothyroidism…
- …but it now has numerous updates throughout where needed, and out-of-date information removed.
- Both adrenals chapters 5 and 6 have been updated, and there’s now details about the use of Adrenal Cortex (ACE), while still having info about hydrocortisone (HC). Chapter 6 now mentions what information applies to either ACE or HC, or BOTH.
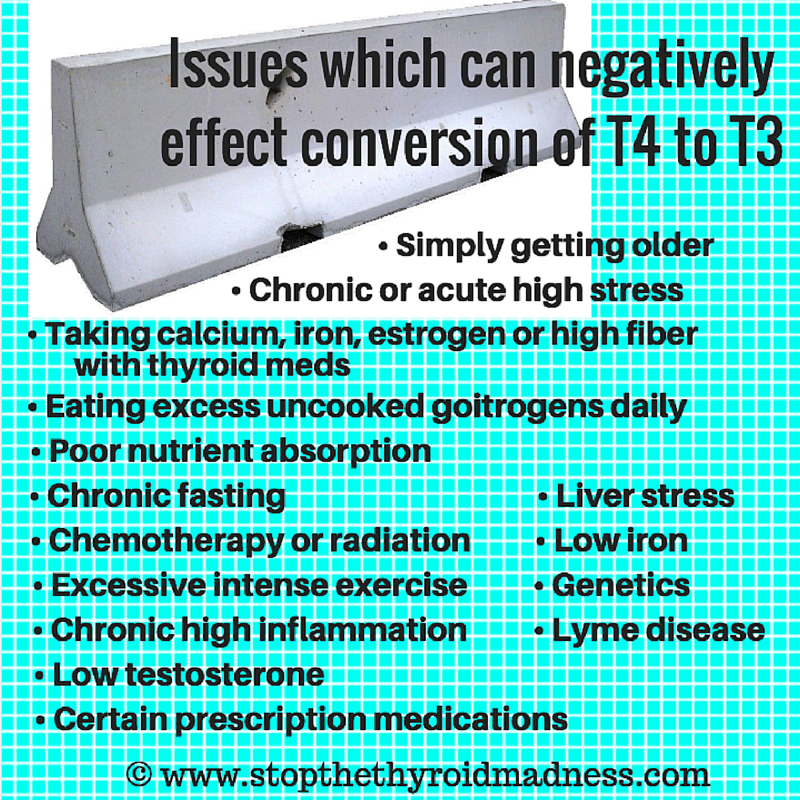
- The T4 chapter now mentions Tirosint, but continues to explain the problem of forcing the body to live for conversion alone. T4-only is T4-only.
- There are now light gray rectangular boxes throughout the book, meant to highlight certain important sentences.
- Emphasis is now on serum iron. i.e. the former book would mention both iron/ferritin, but we now know that it’s far more about serum iron as far as what to make “optimal”. The emphasis about ferritin is more about its ability to reveal inflammation, but can reveal a methylation issue when low with good or high iron.
- There is updated information about
- different kinds of iron products
- better explanations in areas alongside those which were already good
- some new tidbits at the end of some chapters
- some updates to the list of thyroid meds, etc.
- Throughout the book are many more mentions about being “optimal”, not just “on” NDT or T4/T3. It’s also explained often what optimal means in those several places in the book.
- There are great additions to the list of supplements as well as certain foods.
- The chapter on Natural Desiccated Thyroid now has a little photo of an antique bottle of NDT--that’s to show that having T3 in our treatment has been helping patients a long time and safely! This book also mentions the alternative treatment with synthetic T4/T3. Plus various updates throughout while keeping what was always IMPORTANT.
- And there is more.
About HASHIMOTO’S: TAMING THE BEAST…
A “companion book” to the updated revision Stop the Thyroid Madness above
- “Taming the Beast”, a companion book to the updated STTM book shown below, has purposely been put together as concise, yet comprehensive. That means it purposely gets to the point about key information related to Hashimoto’s, while avoiding chattiness or long pages of stories to help those of you with brain fog and concentration problems. 🙂
- Some of the information you may have read before, while some is very unique to this wonderful book!
- FOUR chapters fully pertaining to reported patient experiences and wisdom which can help change your life and reveal that you are NOT alone as a Hashi’s patient!
- Why and how Hashimoto’s patients go years without help or awareness of what is going on
- Patient-reported foods which were and are problematic for some and all the symptoms
- 43 most frustrating aspects of having Hashi’s as expressed by patients (especially about doctors)
- 95 short testimonies on what patients are using or doing to successfully lower their antibodies!
- Like research? You will see a total of 241 footnotes throughout this book that will send you to research articles, or just good information for further reading. Additionally, one chapter simply summarizes 46 research articles pertaining to Hashi’s in one (or two) sentences. And as intended, YOU can choose what you want to further read…or not.
- You will be made aware of, or reminded about, a variety of environmental triggers that can either birth autoimmune Hashi’s in the first place, or make one’s current antibodies worse. (Chapter 4)
- There is a chapter totally focused on Hashimoto’s inflammation--what it can do to you, inflammation labs, what to do about inflammation, supplements and foods to consider to counter inflammation, and short summaries of three ways to eat to counter inflammation. (Plus of course, good footnotes, and added URL’s in the body if needed)
- Two excellent and informative chapters on different gut health problems to explore, or be reacquainted with, including symptoms, types under each category, ways to treat, and more.
- Other examples of patient experiences inserted throughout many chapters
- Different lists of patient-reported symptoms within different chapters to help identify your issues, for example:
- a chapter with symptoms from the autoimmune attack
- another chapter highlighting symptoms of adrenal problems
- more about hypothyroid symptoms that appear while on T4-only or being underdosed due to a doctor’s reliance on the lousy TSH lab test,
- inflammation symptom list…etc.
- Each chapter has a lighthearted small drawing, pertaining to the subject, to send a friendly message about a serious topic, all drawn by Janie A. Bowthorpe, who is an artist.
- There is a blank “NOTES” page at the end of each chapter where you can put page numbers to remember, or additional information you have gleaned in this book or others! That way, you don’t have to flip through all the pages to find what was important to you.
AND SO MUCH MORE!! This book encourages you to underline, highlight, dog-ear, paper clip, and use the NOTES page at the end of each chapter. This is YOUR book.
Laughing Grape Publishing (LGP) now has a brand new, high-end ordering system for the Stop the Thyroid Madness books!!
ORDER: http://laughinggrapepublishing.com